Pathophysiology Of Coronary Artery Disease Health And Social Care Essay
Heart attack has become a common household term in the United States, due to the fact that approximately 16 million American have been diagnosed with coronary artery disease. According to American Heart Association, an American dies every minute due to coronary artery disease. Coronary artery disease also known coronary heart disease or ischemic heart disease encompasses other pathologies, such as angina and myocardial infarction (heart attack). Coronary artery disease occurs when there is a narrowing of the coronary arteries, due to the development of plaques leading to reduce amounts of oxygenated blood to the heart. [2]
Anatomy and Physiology of the Heart:-
The heart is an essential organ that is responsible for pumping blood all throughout the body and supplying it with oxygen and nutrients. It is the central hub for the cardiovascular system and acts as the transport system of the body, which performs via electrical conduction activity. The anatomy of the heart is composed of many structures, such as the four chambers: the right and left atria and ventricles, numerous blood vessels such as the aorta, the pulmonary artery and vein, and the coronary arteries, four valves, three layers of tissue, etc. The aorta is the main artery that pumps the blood out of the heart to the rest of the body; the pulmonary artery and vein transport oxygenated and deoxygenated blood receptively, and the coronary arteries make a crown on the heart muscle and supply the myocardium with oxygenated blood and nutrients. The valves in the heart are responsible for preventing backflow of blood and allow the blood to circulate in an uniform fashion. The electrical conduction system of the heart accounts for the beating of the heart allowing it contract and act as the pump of the body. [2, 3]
Pathophysiology of Coronary Artery Disease:-
When the coronary arteries become occluded due to plaque build up a condition called atherosclerosis occurs. Atherosclerosis means narrowing and hardening of the arteries leading to damage to the blood vessels and is a major contributor to many heart diseases and disorders [4]. These atherosclerotic plaques are formed are from lipid and fat deposits, mainly being cholesterol, which is a reason why diet is also major risk factor in developing coronary artery disease. Arteries are composed of three layers: adventita, intima, and media; the plaque tends to develop between the intima and media layers [5]. These atherosclerotic plaques narrow the lumen of the arteries causing decreased amounts of blood to reach the heart and overtime harden them causing decrease flexibility during vasoconstriction and vasodilatation [4]. Additionally, the atherosclerotic plaques can dislodge causing thrombosis and ischemic events [5]. When the coronary arteries’ function is compromised, the heart does not receive adequate supply of oxygenated blood and nutrients causing decrease cardiac function. At times of stress, the body will try to counteract these changes to achieve homeostasis, by working harder than normal; however, prolonged exertion initiates a cascade to many disease processes and pathologies, such as cardiomyopathy, heart failure, arrhythmias, cardiac arrest, and classically myocardial infarction (heart attack) [4]. Most patients of coronary artery disease experience angina and/or myocardial infarction, or possibly death.
Risk Factors of Coronary Artery Disease:-
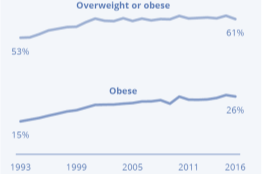
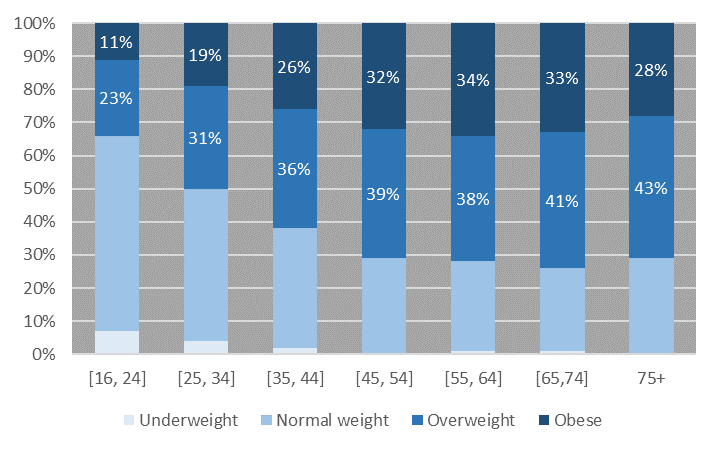
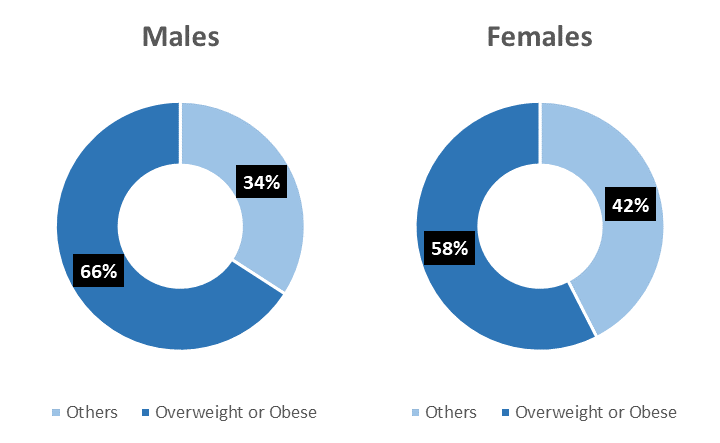
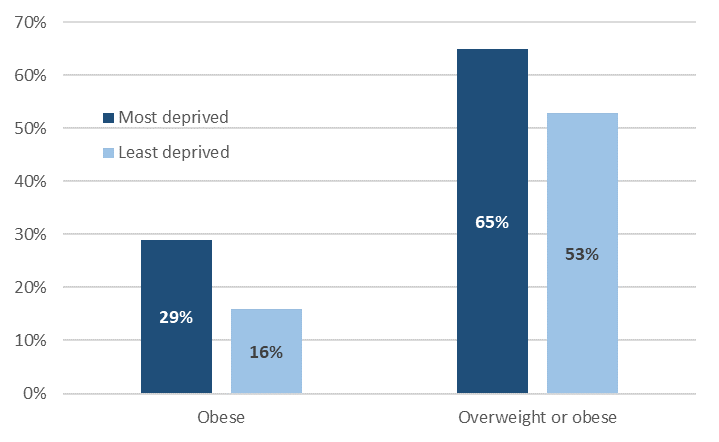
Coronary artery disease tends to be the most common cause of death and disability in the United States. The main risk factors of coronary artery disease are as follows: positive family history, physical inactivity, poor diet, smoking and/or alcohol intake, along with other diseases pathologies like hypertension, diabetes, high cholesterol, and obesity. A person that has positive family history of heart disease of a first degree relative is at greater risk of developing coronary artery disease [2]. Physical inactivity, poor diet, and obesity go hand in hand for developing coronary heart disease. Obesity has become an epidemic that affects one in four Americans and results in many life-threatening consequences. Heart disease has become the cause of death in industrialized nations compare to underdeveloped nations, due to sedentary lifestyle and increased fast-food consumption. The American Heart Association encourages patients to exercise regularly and eat healthy and this also accounts for better prognosis of coronary artery disease even if someone has other risk factors [2]. Research indicates that a diet that’s rich in omega 3-fatty acids, such as fish helps protect against vascular disease [2]. One of the most preventable risk factors for any disease is smoking, and for cardiovascular disease it is the number one preventable cause [2]. The World Health Organization states that 1 year after cessation of smoking, the risk of coronary artery disease decrease by almost half [2]. Additionally, increased age and sex are other contributing factors to coronary artery disease. Statistically, males are more likely to develop coronary heart disease at an early age, however the risk equals for both men and women after post-menopause. Other diseases such as diabetes, hypertension, and/or hypercholesterolemia combined with coronary artery disease results life-threatening consequences, which it is why it’s recommended to keep a close eye on cholesterol, blood pressure and glucose levels and checked on regular basis [2, 4].
Symptoms of Coronary Artery Disease:-
Most patients of coronary artery disease are asymptomatic, whereas other patients can present with a variety of symptoms such as: shortness of breath, tightness around the chest, chest pain, Levine’s sign, or possibly death [2]. Patients that exhibit symptoms tend have advance stages of damage to their coronary arteries [4]. Angina is the classic heart pain most patients complain about that is caused by ischemia. Ischemia is the lack of oxygen supply to a region of the heart [4]. Patients can experience angina at anytime, however classically it’s exhibited after a person has been involved in an extraneous activity, such as exercise. Angina can be categorized as stable, unstable, or Prinzmetal’s (variant) angina [2]. The Levine’s sign is the classic presentation of a heart attack that most actors in Hollywood portray, when they are having a heart attack, which is a clenching fist over their chest [1].
Complications of Coronary Artery Disease/ What is a heart attack?
Myocardial infarction occurs when the heart is deprived of oxygenated blood because of rupture of the atherosclerotic plaque, resulting in a state of ischemia. Supply meets demand theory comes into play, because the heart is demanding oxygenated blood and nutrients, but the coronary arteries are unable to provide due to atherosclerosis build up. The area of the heart that the damage occurs to the heart depends on the vessels that are occluded, exhibiting a variety of symptoms and/or complications [4]. For example, if the myocardial infarction occurs at the right atrium and disturbs the electrical conduction activity of the SA node, it may cause the patient to possibly suffer from arrhythmias. Therefore, essentially if a patient experiences a myocardial infarction at a particular region of the heart that area will suffer an ischemic event and kills the heart tissue hence making it non-functional. Overall, a myocardial infarction has poor prognosis and tends to lead to morbidity and mortality [2].
Diagnosis of Coronary Artery Disease:-
Coronary artery disease is a condition that develops overtime; therefore there aren’t any real tests that can indicate if a person is suffering from coronary artery disease [6]. Healthcare providers use patient’s history, physical exam results, and assess risk factors for developing coronary artery disease [2, 6]. Electrocardiogram, stress testing, echocardiography, and laboratory testing prove to be the test of choice by healthcare providers when examining patients that are at risk of developing coronary artery disease. Electrocardiograms also know as an EKG or ECG detects the heart’s electrical activity, rhythm, heart rate, axis, and any abnormal enlargements of the heart [6]. An EKG is a quick and painless test and can tell healthcare providers if the patient had or is having a myocardial infarction [2, 6]. Stress testing can be induced by exercise or medication for evaluating ischemia in a patient [2]. An echocardiography (echo) utilizes sound waves to monitor the heart’s activity, including the size, shape, and blood flow. Laboratory testing, such as blood tests are conducted on a regular basis to assess the levels of cholesterol, sugar, and proteins such as inflammatory markers [2]. Other tools, such as chest x-rays, angiography, positron emission tomography (PET), and cardiac cauterization can be utilized for patients with greater risk factors and/or advance stages of coronary artery disease [2].
Treatment of Coronary Artery Disease:-
Coronary artery disease is a complex disease since it encompasses other pathologies; however treatment options for coronary artery disease tends to be simple at its early stages, such as lifestyle changes. Patients are encouraged to partake in therapeutic lifestyle changes (TLC), such as daily exercise, eating healthy well-balanced meals, and stress and weight management. A comprehensive TLC plan also helps control other diseases, such diabetes, hypertension and obesity [6]. The American Heart Association recommends patients with risk factors to utilize the DASH diet, which encourages consumption of fruit and vegetables on a daily basis, eating fish twice a week, limiting salt and alcohol consumption [5]. TLC helps reduce the risk of heart disease by lowering cholesterol and maintaining a body mass index (BMI) of less than 25, which is considered to be normal [6]. For advanced stages of coronary artery disease medication such as anticoagulants, aspirin, beta-blockers, calcium channel blockers, and nitroglycerin are prescribed to help reduce symptoms, lower cholesterol and blood pressure, prevent blood clots [2, 6]. Aspirin is the leading medication to help relieve angina and prevent myocardial infarction. Patients that have extensive damage to their arteries or have experienced a myocardial infarction may require medical procedures, such as angioplasty or coronary artery bypass grafting (CABG) [6]. Angioplasty or percutaneous coronary intervention (PCI) is a medical procedure done to open blocked or narrowed coronary arteries [6]. Commonly, people refer this medical procedure as having a “stent” put in, which helps prevent future blockage from occurring. CABG is an extensive surgical procedure done where doctors use blood vessels from other areas of the body that aren’t blocked to bypass narrowed and damaged coronary arteries, thus improving the blood flow to the heart [2, 6]. Overall, patient education proves to be the best treatment option to help prevent coronary artery disease.
Conclusion:-
Levine sign- ^ Edmondstone WM (1995). “Cardiac chest pain: does body language help the diagnosis?”. BMJ 311 (7021): 1660-1. PMC 2539106. PMID 8541748.
Chapter 10 pg 341 CMDT
Human Anatomy and Physiology Chapter 18 pg 662; Marieb/Hoehn
Clinical Pathophysiology made ridiculously simple; Berkowitz
AHA Website- http://www.heart.org/HEARTORG/Conditions/HeartAttack/Heart-Attack_UCM_001092_SubHomePage.jsp
http://www.nhlbi.nih.gov/health/health-topics/topics/cad/