Obesity is a clinical term used to describe excess body fat. The most common method of measuring obesity is the Body Mass Index (BMI). BMI is used because, for most people, it correlates with their amount of body fat. It is calculated by dividing a person’s weight measurement (in kilograms) by the square of their height (in metres). a BMI of 30 or above means that person is considered to be obese (DoH, 2010).
Rising rates –
Obesity is an increasing phenomenon worldwide. In 2008, the Health Survey for England (HSE) data showed that 61.4% of adults (aged 16 or above) in England were overweight and of these 24.5% were obese. They found this was an increase since 1993.
In pregnancy-
In pregnancy the incidence is around 18-19% in the United Kingdom (Kanagalingam et al, 2005).
Between 2004 and 2007, 15% of all UK maternal deaths occurred in women with a BMI of more than 35, half of which had a BMI of over 40. Fifty-two per cent of deaths occurred in women with a BMI of over 25, which is classed as over-weight (Lewis, 2007)
Dangers and complications-
Obesity is a common risk factor in many conditions, especially metabolic (e.g. type 2 diabetes), circulatory (e.g. cardiovascular disease) and degenerative (e.g. osteoarthritis). For women, the risk of gynaecological complications, like endometrial cancer, infertility, menstrual disturbances and ovulation disorders, increase if the woman is obese.
There are many significant risk factors during pregnancy that are affected by obesity. These include early miscarriage, gestational diabetes and pregnancy hypertension/pre-eclampsia (Andreasen et al, 2004/Duckitt et all, 2005/Erez-Weiss et al, 2005/Shaw et al, 2000), venous thromo-embolism and anaesthetic problems, e.g. tracheal intubation or epidural/spinal insertion (Irvine et al, 2006).
If maternal complications develop the fetus/neonate is also at risk of neural tube defects (Shaw et al, 2000), late still birth (Irvine et al, 2006) and neonatal death (Kristensen et al, 2005), fetal macrosomia (Yogev et al, 2005), fetal trauma and neonatal unit admissions (Irvine et al, 2006).
Obesity also causes issues pertaining to the value and reliability of certain aspects of care during the antenatal period. These include difficulties in performing amniocentesis (Irvine et al, 2006), difficulties in achieving venous access, difficulties in performing abdominal palpation (Farrell et al, 2002) and difficulties obtaining ultrasound data for fetal anomalies and growth (Martinez-Frais et al, 2005).
There are significant risk factors due to obesity during the intrapartum period. These comprise increased rates of prolonged labour (Vahratian et al, 2004), risks associated with macrosomia e.g. shoulder dystocia (Irvine et al, 2006/Andreasen et al, 2004), increased rates of operative birth (Irvine et al, 2006/Fraser, 2006), especially for primigravida (Dempsey et al, 2005), difficulties in undertaking instrumental and operative procedures (Irvine et al, 2006/Andreasen et al, 2004) and difficulty siting an epidural or spinal for labour or caesarean section (Irvine et al, 2006).
Postpartum related obesity issues consist of longer post-operative recovery times and increased rates of post-operative complications, e.g. infections of wounds and urinary tract (Irvine et al, 2006). Women who are obese during pregnancy exhibit a tendency to retain fat centrally on their abdomens postnatally, which may results in increased morbidity and mortality later in life (Soltani et al, 2002). Contraception choices will also be influenced by the presence of complications.
Whilst out on my community placement, I was involved in the care of a woman who had a BMI of 52. We were caring for her postnatally after an elective caesarean section. Most likely due to her weight, the surgeon chose to use metal skin clips on her wound, rather than a suture (Irvine et al, 2006). On day five postnatally we were due to remove alternate staples. However, we could see the wound was still gapping and not fused closed so we left them for one more day. On day six we returned and removed the alternate clips with no problem. Irvine et al (2006) recommend an interrupted suture or skin clips on the basis that if a small haematoma or a localised area of infection develops, a few clips/sutures can be removed to aid resolution.
When we revisited the woman on day eight, we found the wound to be very red, oozing puss and giving off a very offensive smell. The woman simply could not get any air to the wound, due to the ‘over-hang’ of her stomach on to the wound. Even whilst lying down, the stomach still covered the area if it was not held up and supported.
I feel this was an important factor to her getting a wound infection. Due to the over hanging of the pannus, women are significantly at increased risk of wound infection even if given postoperative prophylactic antibiotics (Irvine et al, 2006).
Discuss differing health promotion strategies according to context of the case study
Obesity levels in England have currently reached epidemic levels and Suffolk is consistent with this. Suffolk is below the average obesity level, but this varies across the county (Transforming Suffolk, 2008).
A new project has been launched, called Healthy Ambition Suffolk to make Suffolk the healthiest county in the UK by 2028. Part of this includes tackling obesity.
Governments – 5 a day scheme
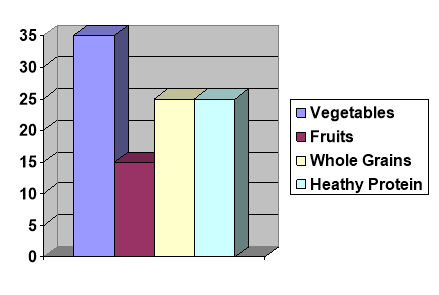
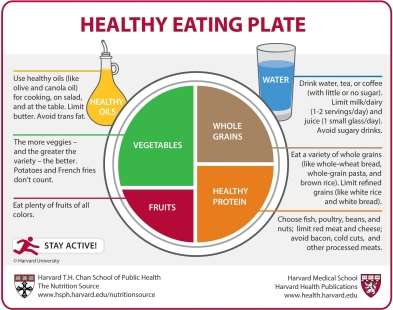
In January 2009, the Government began a campaign in response to the rising rates of obesity. Change4Life is England’s first ever national social marketing campaign to promote healthy weight and supports the overall Healthy Weight, Healthy Lives strategy. One of Change4Life’s recommendations is to eat 5 A DAY as part of a healthy balanced diet (DoH, 2010).
Eating at least five portions of fruit and vegetables everyday seems valuable, however it is hard to see exactly how this will help with the fight against obesity, unless it is thought that consuming more fruits and vegetables will transfer calories from other sources.
Healthy start vouchers
The Government has also introduced another health promotion strategy called Healthy Start. This consists of vouchers with a monetary value which can be used against fresh fruit and vegetables, fresh milk and also infant formula. Not every woman will be able to claim these, they are income assessed and women need to fit certain criteria (DoH, 2006).
Dietian/nutritionalist referrals
In accordance with the National Institute for Health and Clinical Excellence (NICE, 2010), pregnant women with a body mass index of more than 30 will be under consultant led care and receive any additional care they require.
Midwives should refer women to a dietician for assessment and advice on healthy eating and exercise. However, they should not recommend weight-loss during pregnancy (NICE, 2008).
In 2003, a report on obesity by the House of Commons demanded six other government departments joined forces. These departments were:
Department of health: Main responsibility as obesity is a public health issue.
Department of culture, media and sport: For promoting sports and physical activity.
Department for education and skills: To ensure that children get adequate physical education at schools and have access to food at schools.
Department for transport: For making ‘healthy’ transport policies to encourage cycling and walking.
Department of environment, food and rural affairs: For farming and produce of healthy food.
Department of trade and industry: For food manufacturing and retail industry
Analyse concepts of poverty, disadvantage and inequality and the impact on childbearing women, babies and their families.
There is evidence that maternal obesity is related to health inequalities, particularly socioeconomic deprivation, inequalities within ethnic groups and poor access to maternity services (Heslehurst et al 2007). Healthy food is often more expensive and gyms facilities and fitness classes are not readily available for low income families.
Analyse and reflect upon the role of the midwife and other professionals in their contribution to the public health agenda
The Faculty of Public Health define public health as “the science and art of preventing disease, prolonging life and promoting health through organised efforts of society”
(Acheson, 1988). Public health is about promoting physical, mental or emotional well-being by inspiring, educating and empowering the public to stay healthy (CSP, 2010). Midwives play a very important role in achieving this. When initially booking women for their pregnancy care, if there are any health concerns the midwife should advise and refer to other health professionals if necessary.
The role of the midwife has evolved in recent years with more emphasis on a
public health role (DoH, 1993).
It is reasonable to expect that midwives should have a working knowledge of the effects obesity, as well as other common public health issues, including teenage pregnancy, drug and alcohol abuse and smoking. They should have an understanding of the common risks associated with obesity and what they should be able to offer by way of support (English National Board, 2001).
The Saving Mothers’ Lives report (2003-2005) carried out by the Confidential Enquiry into Maternal and Child Health (CEMACH) recommends that obese women should receive help to lose weight prior to conception. However, this is not always possible.
I believe the Government are currently taking the correct steps to combat obesity. Whilst working on community and undertaking booking appointments, I have not actually seen women being referred for high BMI’s. This is due to my Trust not taking a woman’s height and weight at the booking appointment so their BMI is unknown. These details are recorded when the women go for their 12 week dating scan. Therefore, referrals for high BMI’s are carried out from the antenatal clinic.
As midwives, we are used to managing women with complex needs in partnership with other agencies. I believe it is working within the multi-disciplinary team which gives the best care to women.
The Royal College of Midwives (RCM) surveyed midwives and new mothers, which were published during Midwifery Week 2008. They showed that due to the shortage of midwives women are being short-changed on essential public health services and advice and are not getting the level and quality of service needed in areas such as obesity, smoking cessation, breast feeding and alcohol intake.
The level of help that obese pregnant women are receiving is a cause for concern. Only 8% of women were offered help and advice, while the amount of women who said they would have liked to have had the service was 30%. The midwives surveys supported these findings, with only a fifth (22.5%) stating that they are able to offer or run obesity clinics, and 71% saying their Trust do not run them (RCM, 2008).